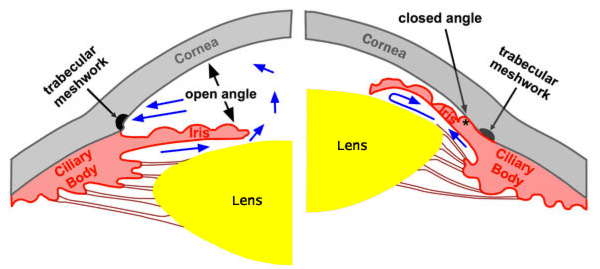
In angle closure, fluid in the eye is unable to drain from the trabecular meshwork, resulting in the build up of eye pressure
The front of the eyeball is filled with a colourless fluid, known as aqueous humour. It is continually being produced in the eye and drained from the eye, through a drainage channel in the eye called the trabecular meshwork. In some patients, the part of the eye where the trabecular meshwork is located (known as the angle) is narrow, which can reduce the drainage of fluid from the eye. When pressure builds up in the eye as a result of this, angle closure glaucoma results.
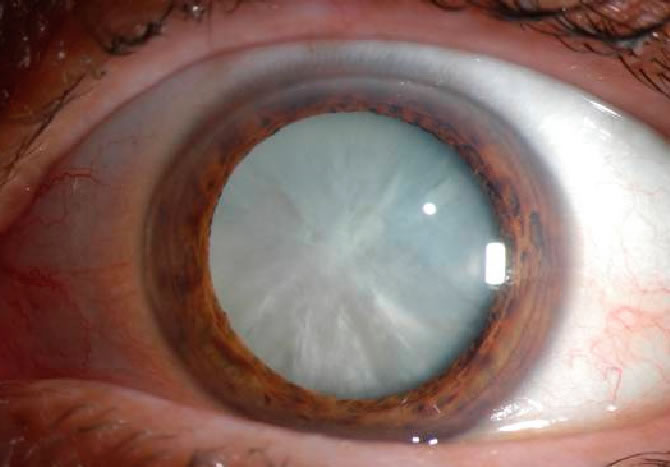
Pressure build up can occur acutely, and can build up to very high levels. This results in symptoms of eye pain, redness, blurred vision and headache. The patient may also experience nausea and vomiting.
The red, painful eye of acute angle closure glaucoma
Angle closure glaucoma is an emergency. When the eye pressure is dangerously high, the optic nerve located at the back of the eye can become damaged. This damage is permanent and irreversible, and the patient can permanently lose vision as a result.
How is this condition treated? In the acute situation, the priority is to lower the eye pressure as quickly as possible, to reduce the damage to the nerve. This is achieved using medications, which are administered as eyedrops, oral pills or even injections.
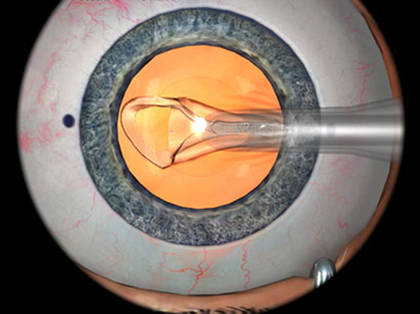
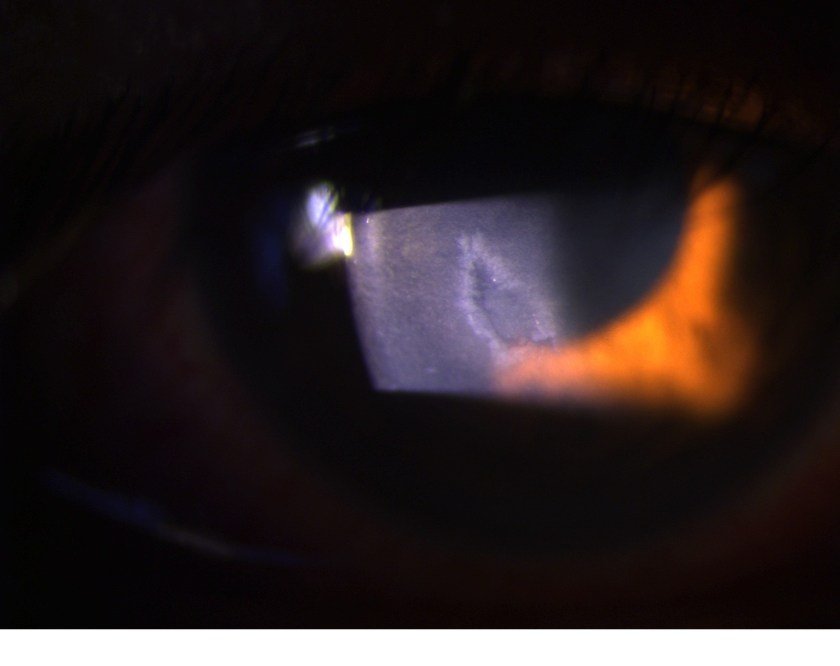
Once pressure is controlled, laser treatment is performed to create an alternative channel for fluid to flow, and prevent the build up of pressure from occurring again.
Laser treatment has been performed in this eye, creating an alternative channel for fluid to flow and preventing acute pressure rise from recurring
Patients with this condition sometimes suffer damage to the trabecular meshwork as a result of the high pressure, which results in chronic angle closure glaucoma. These patients often require life long treatment with anti glaucoma eyedrop medications.
Eye pain and redness are symptoms that should never be ignored, especially if they are accompanied by headache and vomiting. If you ever experience these symptoms, consult an Eye doctor without delay.
In Singapore, the overall prevalence of glaucoma is 4%- meaning that in your lifetime, you have a 4% chance of developing glaucoma. Not a big number- the odds are still in your favour, but it is still a condition worth knowing about.
Open angle glaucoma accounts for nearly half of glaucoma in Singapore- 1.7% of the population have or will have this disease. That figure does not sound intimidating. What is worrisome is that this disease does not have many symptoms, and many patients are diagnosed late for this reason.
In open angle glaucoma, the optic nerve at the back of the eye undergoes progressive damage. This is most often (but not always!) due to high eyeball pressure. Contrary to popular belief, this rarely causes pain or discomfort to the eye, and the patient is often unaware that he has glaucoma.
The result of optic nerve damage is visual field loss- reduction in the patient’s peripheral vision. Peripheral vision is important in daily life- it allows us to safely cross roads or drive, for example, but early peripheral vision loss is usually not noticeable. A loss of central vision is noticed by patients immediately, but loss of peripheral vision is much more subtle and can progress to severe loss before it is perceived by the patient.
As a result, open angle glaucoma is often diagnosed late, when significant peripheral field loss has occurred. Occasionally patients present when only tunnel vision remains, or worse, when the peripheral field is completely lost and the disease starts to affect central vision.
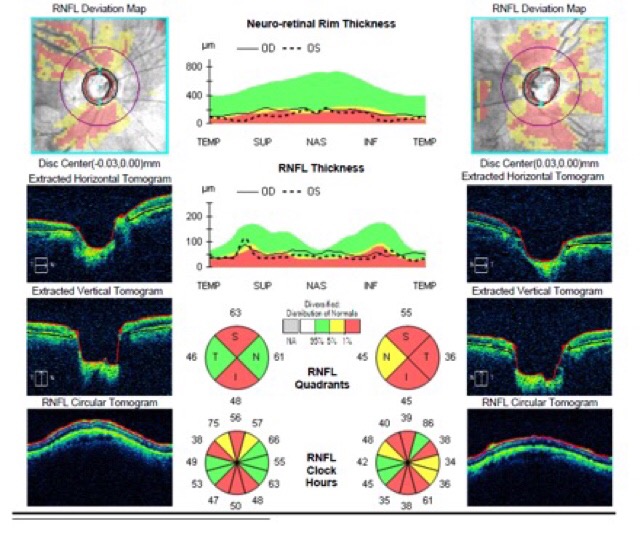
How is open angle glaucoma diagnosed? When patients present to an Ophthalmologist, a detailed history and physical examination is performed. Intraocular pressure is measured- usually raised beyond 21mmHg in the case of open angle glaucoma. Signs that point to the disease- a characteristic weak, thinned-out appearance of the optic nerve, would make one suspicious of the disease. The disease is often confirmed on further testing, where both structure and function of the nerve is tested. High resolution Optical Coherence Tomography (OCT) scans of the optic disc and the surrounding nerve fibre layer can determine if there is any thinning of the nerve due to glaucoma, and Humphrey Visual Field (HVF) testing can map out areas of visual field loss.
High resolution OCT image showing significant nerve fibre layer thinning. The red areas in all the circular plots are abnormal.
How is open angle glaucoma treated? Several eyedrop medications exist that can be instilled to lower intraocular pressure and reduce the progression of nerve damage. If eyedrops are insufficient to treat the disease, laser procedures and surgery can also be done to manage the disease.
If you are over the age of 40, or have a family member who has glaucoma, it is a good idea to go for a comprehensive eye screening to ensure that you do not have this problem.
I have been a cataract surgeon for over a decade now, and with that experience, I am usually fairly accurate in my clinical assessment of how well my patient will fare after surgery. Occasionally I am surprised myself by the outcomes, just like I was on a case I operated on last week.
Mdm C is not your typical patient. She presented to me with poor vision in the right eye, and on examination she did indeed have a cataract in that eye. However, she was also markedly short sighted in that eye, and had been so since childhood. Her spectacle degree in that eye was 750 degrees, with astigmatism of 225 degrees. Her vision was perfect in the left eye without glasses. Due to the large imbalance between spectacle degrees of both eyes, she had lived her life without glasses and relied heavily on the left eye, and had lived with poor vision in the right eye for decades.
In this case, there is a high chance that she has developed a lazy eye in the right eye. In childhood, vision must be good in both eyes in order for pathways between the eye and brain to develop normally. If vision is better in one eye, the poorer eye will become “lazy” and the pathways to the brain will not develop normally. This is a condition known as amblyopia. Pathways mature when a child reaches the age of 8, and beyond that age, the vision in the lazy eye cannot be improved.
In Mdm C’s case, I felt that the likelihood was high that she had amblyopia in the right eye, as she had been highly short sighted in that eye all her life. As a result, even with cataract surgery, I felt her vision would not be as good as her left eye.
I discussed this at length with her and her son, explaining to them the benefits and risks of cataract surgery, as well as my concerns that her vision would not be perfect in the right eye even after surgery. However, as her vision in the right eye was very poor, she decided to proceed with surgery despite the guarded prognosis. Her vision was 6/120- she was only able to see the biggest letter on the chart.
Surgery proceeded uneventfully. I removed the cataract and implanted a toric intraocular lens in the right eye, which corrects for both short sightedness as well as astigmatism.
She returned for review on the first postoperative day. When I opened her chart, I thought I had the wrong patient. Her vision in the right eye was 6/6- perfect vision!
Mdm C was ecstatic. She had not seen well in the right eye for decades as it had always been highly short sighted, and had never worn glasses or contact lenses in that eye. For the first time in her life, she had good vision in both eyes.
I had been wrong about my assessment that she had a right lazy eye- and I had never been so happy to have made a misdiagnosis.
I am always delighted when my patients achieve good outcomes, there is nothing more satisfying to me than restoring vision to my patients. When outcomes exceed expectations, I can only be humble and grateful, to God for whom nothing is impossible, and to my patients, for putting their faith in me, and giving me the privilege of being their cataract surgeon.
I have come to realise that glaucoma is a very poorly understood condition. Most people have heard of the disease, but few understand what it really is and how it can affect them. In this article, I will attempt to explain what glaucoma is.
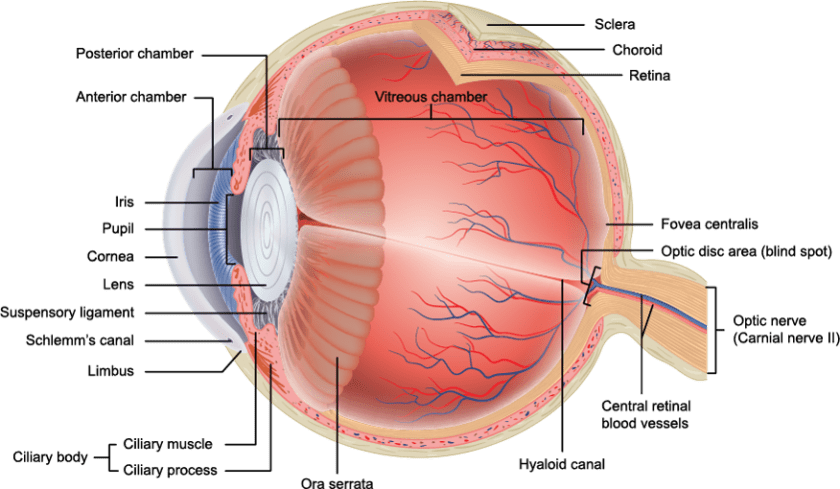
Glaucoma is actually a disease affecting the optic nerve of the eye. Images are perceived by the retina and carried via the optic nerve to the brain, where they are interpreted. Hence, the optic nerve is a very important structure, and its health is critical to having good vision.
Glaucoma results in damage to the Optic Nerve, which connects the Eye to the Brain. Without a healthy Optic Nerve, we cannot have good vision.
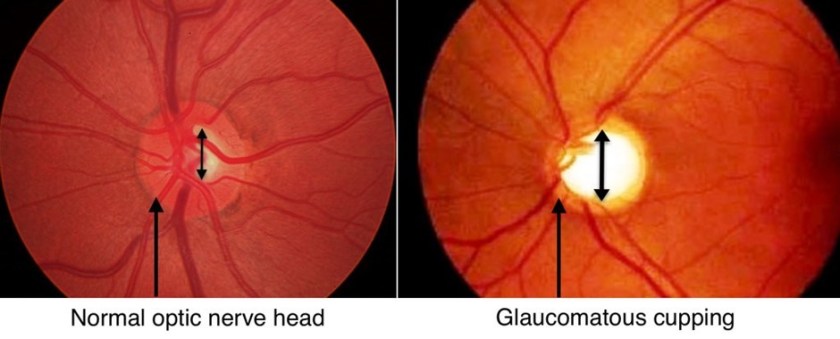
In glaucoma, the optic nerve is progressively damaged, and this affects both its structure and function. Structural damage of the nerve can be seen by an Ophthalmologist using special instruments to visualise the inside of the eye. Structural damage can also be measured objectively with specialised tests that can be done in an Ophthalmologist’s clinic.
Structural damage to the Optic Nerve results in what is known as cupping of the nerve, where its edges are thinned out like the rim of a cup.
Functional damage to the nerve typically results in a loss of ones’ peripheral vision, which can progress from mild loss to tunnel vision. Interestingly, although peripheral vision is very important, mild losses are usually not noticed by patients. For example, when I see something out of the corner of my eye (such as a car on the road), my instinct is to turn my head in the direction of the car, thereby bringing it into my central field of vision. Hence, if my peripheral vision is poor, I may not initially realise it.
Here’s an illustration I found that shows what tunnel vision is.
The cause of the optic nerve damage is frequently (but not always) raised eyeball pressure, and hence the strategy to treat glaucoma involves lowering the eyeball pressure. This is usually achieved with medications, but may also involve laser treatment or surgery.
Here’s one fact that is quite frightening- most cases of glaucoma have no symptoms! Normal eyeball pressure is about 21mmHg, and contrary to popular belief, eyeball pressure can be raised without pain or other symptoms. A patient usually only feels eye pain when eyeball pressure is very significantly elevated. Unfortunately, in most cases, eyeball pressure is raised but not to the extent that it causes pain, and optic nerve damage goes undetected until late stage disease. Patients sometimes present with only tunnel vision remaining, and because optic nerve damage cannot be reversed, there is no way to restore their peripheral vision once lost.
How do we know that we do not have glaucoma? Since glaucoma has no symptoms, the only way to know for sure is to see an eye care professional for eye screening. Annual eye screening is recommended for anyone over the age of 40, to detect eye conditions such as cataract and glaucoma.
I hope this gives you a better understanding of what glaucoma is! There are actually many types of glaucoma, and many different types of treatment, which I will share in subsequent posts.
Have you ever fallen down and scraped your knee or elbow? I was an active kid who spent most days after school climbing trees and riding my bicycle around the neighborhood, and came home with abrasions on my knees many many times. Remember how painful they were?
Imagine the skin of the eye getting an abrasion like your knee. This can happen from relatively trivial trauma, like a scratch from your fingernail or being brushed by a tree branch. The cornea is the surface layer of the eye and it has a skin layer similar to the skin on our bodies, but has 5 times the number of pain receptors per square mm compared to the skin on your body. For that reason, cornea abrasions are exquisitely painful.
See the faint triangle shape on the cornea surface? That’s the outline of a cornea abrasionThe same abrasion seen under higher power magnification
Fortunately, the abraded cells grow over very quickly with appropriate treatment, and the patient feels relief of the pain within days. However, the problem doesn’t always end there.
Unlike the skin on your body, which heals completely relatively quickly, the skin on your cornea takes a long time to heal completely. New cells grow over to cover the abrasion in a matter of days, but these cells are immature and don’t stick well to each other. It takes a period of months to years for these cells to mature and stick firmly to each other. In the meantime, patients are at risk for recurrent cornea erosions.
When the cells are immature, minor trauma can cause the sheet of cells to detach from the cornea, and the patient sustains a cornea abrasion all over again. Sometimes the trauma is nothing more than the patient opening his eyes in the morning- the movement of the eyelid over the immature sheet of cornea cells is enough to cause the abrasion to happen!
Although it is a painful and troublesome condition, recurrent cornea erosions can be treated. Patients will require plenty of eyedrops and ointments to lubricate the eye, especially at night, and usually for many months to years. If the condition recurs over and over again, additional treatment such as specially fitted contact lenses or laser treatment can be considered.
Happy New Year! It is the time of the year to take stock of our lives and perhaps make little changes that might be good for ourselves. Here are a few little changes you can make to make your Eyes happier this new year.
Take concrete measures to reduce your screen time! This year I have decided to shift my phone charger from the bedside table to the opposite corner of my bedroom, so that I will not use my phone in bed. Smart phones emit blue light, which recent studies suggest may cause retina damage and contribute to the formation of age related macular degeneration.
Less screen time=more time for what’s important in life
Spend more time with your kids outdoors. Time spent outdoors has been shown to help prevent the onset of myopia in children. I have 2 young ones myself, and I bought them pool floats for Christmas last year, to encourage them to spend less time in front of the TV and more time goofing off in the pool.
Goofing off in the pool!
Eat more fish. Deep sea fish such as salmon and tuna contain omega-3 fatty acids, which has a host of Eye benefits. Omega-3 fatty acid consumption can improve the symptoms of dry eyes, and may also help prevent age related macular degeneration. Other good sources of omega-3 fatty acid include flaxseed, walnuts and deep green leafy vegetables. I don’t know about you, but I don’t need much persuasion to eat more sashimi!
This was dinner a few nights back- quick, delicious and so good for you!
Have a great year! Be good to yourself, and be good to your Eyes too.
I was recently asked to see a patient in the ICU. This patient was admitted for lymphoma and had developed a reaction to a drug she was taking. The reaction can also affect the Eye, and hence I was asked to review her.
She reminded me of a patient I operated on a few years ago. Mr X was an elderly gentleman who had end stage multiple myeloma and had been given 6 months to live. His Oncologist referred him to me because he had poor vision.
I examined him and found that he had significant cataracts in both eyes, causing his vision to be quite poor. I was hesistant to offer him cataract surgery because he did not have long to live, and didn’t have much time to reap the full benefits of cataract surgery. I did not want him to spend his time and his money on surgery if he had more fulfilling ways to spend the limited resources he had left on earth.
He assured me that surgery was what he really wanted. He told me, “Doctor Chan, I do not have much time left. I just want to see my loved ones clearly in my last days. Will you help me?”
We scheduled surgery a few days later. Cataract surgery is always done one eye at a time, and I arranged for the worse eye to be done first. I also thought that if I restored vision in the worse eye, perhaps he would be satisfied and may not want to proceed with the second eye.
Surgery went well and was uncomplicated. On the first postoperative day, he could see 6/6- perfect normal vision. He was elated. The first question he asked me was, “Doctor Chan, when can we do the second eye?”
I could not refuse him. We scheduled surgery 2 days later.
Mr X had a good outcome for the other eye as well, and achieved 6/6 vision in both eyes for distance. As I had implanted monofocal intraocular lens implants for both eyes, he required reading glasses to read, but was happy with the outcome.
His gratitude was palpable. He said, “Thank you Doctor Chan, you have made a dying man very happy”.
I reviewed him again a week after surgery, and again a month later. He was subsequently discharged to a hospice that cared for him in his final days. He did not show up for the appointment I made for him 6 months after surgery.
Every patient is special to me, I cherish each and every one of them, and I am always humbled by the privilege to help them. Mr X, however, reminded me what I studied Medicine for, why I worked so hard as a trainee to become an Ophthalmologist, and what debt I owe society for the privilege of being a doctor.
Mr X, I will always remember you. Thank you for the privilege of being your cataract surgeon. I am grateful for the trust you had in me. It was my great honour to have helped make your last days brighter and more comfortable. May you rest in peace.
Have you or anyone you know ever had one of these?
Chalazion is an extremely common condition- in my practice, I see several cases per week. It is essentially a mild condition, but causes significant distress because they cause swelling of the eyelid and are extremely visible. If you or anyone you know has ever had a chalazion, here’s five things you may not have known about the condition:
They are not caused by infection
A chalazion presents as a red swelling on the eyelid, and many assume it is caused by an infection of the eyelid. Some joke that it is caused by looking at attractive members of the opposite gender! On the contrary, a chalazion is formed when the opening of an oil gland at the base of an eyelash gets blocked with dirt. The oily secretions of the gland get trapped behind the blocked opening, and result in a swelling on the eyelid.
Although generally sterile, chalazions can become infected if left untreated or if the overlying skin is broken. This can result in severe eyelid swelling and pain, and needs to be treated with antibiotics without delay.
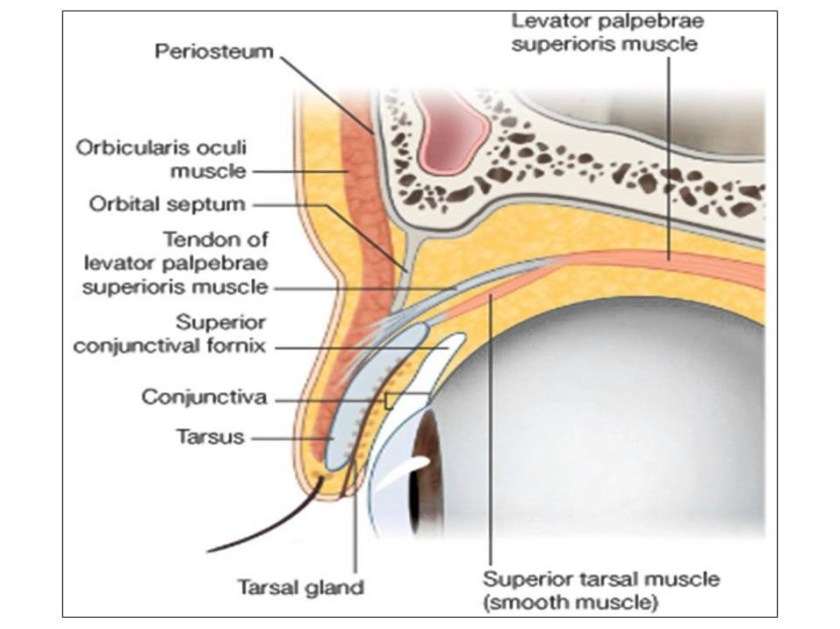
A chalazion forms when the tarsal gland, which secretes oil onto the tear film, gets blocked by dirt. The oily secretions become trapped and a swelling results.
They can happen at any age
Chalazions happen in both young and old, because the oil gland openings can become blocked at any age. However, if a chalazion keeps recurring at the same spot on the eyelid of an elderly person, the possibility of an eyelid cancer needs to be borne in mind, and a biopsy of the eyelid should be performed.
Small chalazions can be managed without the need for a surgical procedure
Small chalazions may be amenable to conservative treatment. Warm compresses should be applied twice a day to the affected area, with the hope that the warmth can cause the gland opening to dilate and allow trapped secretions to be released. However, if the chalazion is longstanding, secretions tend to harden and are thus impossible to release from a small gland opening. In those cases, a small surgical procedure may be required to release the trapped oily secretions.
If a surgical procedure is required, it can be done without a scar
The surgical procedure is done under local anesthesia in an Ophthalmology clinic. No sedation or general anesthesia is required. After injection of a pain killer medication under the skin of the eyelid, a clamp is applied to the eyelid to reduce bleeding. The eyelid is then everted and an incision is made on the underside of the eyelid. Trapped secretions are then removed through the incision. As the incision is made on the underside of the eyelid, no visible scar remains after the procedure is over.
During the surgical procedure, a clamp is applied to the eyelid and the lid everted, so that the incision can be made on the underside of the eyelid. This way, there is no visible scar on the skin.
Regular maintenance is required to prevent them from recurring
It is important to maintain a routine of eyelid cleansing, in order to prevent oil glands on the eyelash margin from becoming blocked. An Ophthalmologist typically prescribes an eyelid cleaning solution or wipes, which should be used twice daily to remove all dirt from the eyelid margin that may cause glands to become blocked.
I hope this has been useful to you. Do let me know in the comments if there are other topics you would like me to cover!
I am very honoured to be the first Oculoplastic Surgeon to practice in Farrer Park Hospital! I commenced practice at the International Eye Cataract Retina Centre there this week, and I just love it- it is a beautiful, brand new hospital with excellent facilities. Do drop by to visit anytime!
I have been asked what exactly Oculoplastic Surgery is. To put simply, it is the medical and surgical treatment of conditions affecting the eyes and surrounding areas. Most of my Oculoplastic work revolves around treating eyelid problems, eye socket problems and tearing problems, especially those due to tear duct blockage.
Eyelid surgery is done for both medical and aesthetic reasons. Eyelid lifts can be done for hooded eyelids, eyebags and droopy eyelids, and can significantly improve one’s quality of life, especially if the eyelid is blocking vision. Other eyelid problems amenable to surgery include eyelashes turning inwards (entropion), turning outwards (ectropion), and growths on the eyelid.
There are also conditions that affect the eyelids that do not require surgery and can be treated with medicine or injections. These include twitching eyelids, half face twitching, and age lines around the eyes- frown lines, laugh lines/crow’s feet, forehead lines.
Eye socket problems include growths in and around the eye socket, eye problems due to thyroid gland diseases, and fractures of the eye socket due to trauma.
Tearing is a very common symptom, and has a myriad of causes. One of the causes is a blockage of the tear duct, which can cause infection in addition to tearing. It can be treated by surgery, which can even be done through the nose, without any visible scars.
I hope this gives a quick overview of the scope of Oculoplastic Surgery! I am very privileged to be a practitioner in this field, it is a fascinating subspecialty with many different surgical techniques, and each treatment has to be customised to the patient’s needs because everyone’s anatomy is different. It is challenging and deeply satisfying work.
Have you or anyone you know been diagnosed with a cataract and are contemplating surgery for it? I have done well over a thousand cataract operations in my career, but I have to be honest- I have never been on the other side of the table, and have never had the procedure done myself. A good friend (an Anesthetist I have worked with for many years), however, has had both his cataract surgeries done, and I made him give me a blow-by-blow account of the experience, so that I could better understand what my patients go through. Here’s what to expect on the day of surgery.
This Eye badly needs Cataract Surgery!
The Preoperative Preparation
If asked to fast before surgery, please do fast! Please do not cheat and eat if instructed not to do so. During surgery, mild sedative medications may be given to you if you feel anxious, to calm your nerves for a better surgery experience. It is important that these medications be given on an empty stomach, in case you feel nausea and retch- regurgitated stomach contents can actually go down the breathing tube and cause serious lung problems! Fasting is usually from 12 midnight the night before for surgery listed in the morning, and from 6am on the day of surgery for surgery listed in the afternoon.
You will be asked to report early for surgery because preoperative eyedrops have to be instilled into the eye, to prepare the eye for the cataract operation. These drops are needed to dilate the pupil of the eye to allow the cataract, which lies behind the pupil, to be removed. Drops usually take about an hour to reach peak effect.
Before and After Pupil Dilation
The Surgery Experience
Once ready, you will be taken to an operating theatre. If you have requested for an Anesthetist to be present, he or she will set a line on the back of your hand- this is used to administer sedative medications to relieve your anxiety and make you more calm.
The Eye itself requires some anesthetic for surgery as well, and this is usually administered via eyedrops. Your surgeon will usually administer these drops him/herself. Occasionally, an injection may be required to achieve complete numbness of the eye. This is given just below the eye, through the skin on the lower eyelid. It sounds intimidating, but really only takes a few seconds to give and it is over!
Surgery is done on an operating table, with the help of an operating microscope. Once your face has been cleaned and a sterile surgical draped placed over you, a small metal speculum will be used to help to keep your eye open throughout the surgery. The speculum will cause mild discomfort and a feeling of pressure around the eye- do alert your surgeon if the discomfort is unbearable, as the speculum can be adjusted to your comfort.
The Speculum- uncomfortable, but not as bad as it looks I promise!
Once surgery starts, you will be asked to look straight ahead at the microscope. What you will see is 3 bright lights arranged in a triangle. Although it is difficult to maintain your focus on the 3 lights – the body’s instinct is to close the eye, it is imperative that you try your best to focus on the lights during surgery.
You will first feel mild pressure as the surgeon makes 2 incisions in the cornea (the transparent tissue in the front of the eye), and makes a small hole in the capsule of the cataract. Some water is injected around the cataract to loosen it, then the ultrasound (phaco) probe is inserted into the eye.
When the probe is activated, a buzzing sound is heard, and this sound is usually interspersed with higher pitched sounds as varying amounts of ultrasound is applied to break up the cataract. Do not be alarmed by the machine noises, they are perfectly normal!
Once the cataract has been removed, the intraocular lens has to be inserted in its place to give you good vision after the surgery. I have been told that this is the most uncomfortable part of the surgery. Intraocular lenses are small, foldable acrylic or silicone implants that are injected into the eye through the main incision. The lens is usually about 13mm long and 6mm wide, but has to squeeze through a tiny 2.65mm incision, hence the patient usually feels the most pressure as in enters the eye. Thankfully, lens insertion is usually over in a matter of seconds.
Intraocular lenses are folded and injected into the eye via a small 2.65mm incision
Once the lens has been inserted, surgery is more or less done! What remains is to instil medications into the eye, ensure the wounds do not leak (they generally are self sealing and do not need to be stitched), and the operation is over.
In some circumstances, additional steps such as the use of a Femtosecond Laser or a Computer Guided Toric Lens Placement system may slightly prolong surgery. More about these exciting technology in another post!
What will I see and hear during Surgery?
Patients are often fearful that they will see instruments going in and out of their eyes. In fact, this is not the case. Usually what is seen at the start of surgery is the 3 bright lights of the operating microscope. These 3 lights gradually become a bright blur as surgery progresses, and even at the end of surgery when the drapes are removed, vision is not clear. This is because the light-sensitive pigment in the retina of the eye gets bleached by the microsope light, and regeneration of the pigment requires some time in a dimmer environment. Hence, you will only begin to see clearer in the recovery room after surgery is completed.
The operating theater is a busy working environment the Surgeon, Anesthetist and Nurses work together to perform the operation on the patient. In addition to the beeps and buzzing of the machines, you can expect to hear people talking- the Surgeon requesting for instruments from the Scrub Nurse, the Anesthetist giving instructions to his Nurse. Your Surgeon or Anesthetist may even talk to you, to keep you calm and keep you company during your surgery!
What happens Postoperatively?
Once surgery is over, you will be brought to a recovery room to be monitored. Patients are often fasted for surgery and come out pretty hungry, so milo and cookies are served! After the nurses have shown you how to instil your postoperative eye drops and care for your eye, you can be discharged to go home.
The postoperative hot beverage and cookies- something to look forward to after surgery!
I hope this has been a useful guide on what to expect from Cataract Surgery! Many of my patients are intimidated by the prospect of surgery, but come out the other side surprised by how pain-free and simple the process is. Do write to me if you have questions, I will be glad to answer them.













 I was recently asked to see a patient in the ICU. This patient was admitted for lymphoma and had developed a reaction to a drug she was taking. The reaction can also affect the Eye, and hence I was asked to review her.
I was recently asked to see a patient in the ICU. This patient was admitted for lymphoma and had developed a reaction to a drug she was taking. The reaction can also affect the Eye, and hence I was asked to review her.



 I am very honoured to be the first Oculoplastic Surgeon to practice in Farrer Park Hospital! I commenced practice at the International Eye Cataract Retina Centre there this week, and I just love it- it is a beautiful, brand new hospital with excellent facilities. Do drop by to visit anytime!
I am very honoured to be the first Oculoplastic Surgeon to practice in Farrer Park Hospital! I commenced practice at the International Eye Cataract Retina Centre there this week, and I just love it- it is a beautiful, brand new hospital with excellent facilities. Do drop by to visit anytime!